
Summary of recommendations for quality of care in cataract surgery management – WHO
Raising the Bar in Cataract Surgery.
A Practical Framework for Quality of Care
Cataract remains the leading cause of blindness worldwide, affecting an estimated 94 million people aged 50 years and over who could benefit from surgery. In response to this enormous and growing burden, the World Health Organization has set a global target to increase effective cataract surgical coverage by 30 percentage points by 2030. Crucially, “effective” coverage means not only expanding access, but ensuring high-quality outcomes.
The WHO Summary of recommendations for quality of care in cataract surgery management provides a structured, evidence-informed framework to strengthen quality across the entire surgical pathway.
This blog post distills the key recommendations of the document into a practical roadmap for policy-makers, program managers, and surgical leaders.
I. Preoperative Phase. Laying the Foundation for Success
Quality cataract surgery begins long before the first incision. The WHO emphasizes that strong preoperative processes are central to both safety and visual outcomes CATA 9789240121089-eng.
1. Comprehensive Assessment
A thorough medical and ophthalmic history is mandatory. This includes prior ocular surgeries, systemic conditions, allergies, and medication use.
Every patient should undergo a comprehensive eye examination. Preoperative visual acuity and best corrected visual acuity must be documented. Cataract diagnosis should be based on symptoms such as glare and blur, not visual acuity alone.
Ocular comorbidities that may affect outcomes must be identified and managed in advance. Complex cases requiring specialized equipment or higher surgical expertise should be anticipated and prepared for accordingly.
2. Systemic Health Optimization
Active infections must be treated before surgery. Blood pressure and blood glucose must be within acceptable limits. Uncontrolled systemic disease should be stabilized to reduce perioperative risk.
3. Informed Consent and Patient-Centred Care
Personalized counselling is essential. Patients must understand the type of anaesthesia, expected outcomes, intraocular lens options, risks, and postoperative expectations. Consent forms should use plain language and ensure comprehension, including translator support when necessary.
This reinforces one of WHO’s core quality principles. Care must be people-centred.
4. Biometry and IOL Planning
Reliable axial length and keratometry measurements are mandatory. Optical biometry is preferred when feasible. Equipment must be properly maintained and calibrated.
IOL selection should consider patient goals and visual preferences whenever possible.
5. Antibiotic Use Before Surgery
Routine preoperative topical antibiotics are not recommended.
II. Intraoperative Phase. Standardization, Safety and Skill
The intraoperative period demands rigorous adherence to safety standards and procedural discipline.
1. Operating Theatre Standards
Sterilization must comply with national and international standards. Infection control processes should be integrated into broader hospital programmes.
Key requirements include safe theatre design, ventilation systems, sharps disposal, backup power supply, and documentation of sterilization processes.
2. Infection Prevention
Povidone-iodine or chlorhexidine must be applied prior to surgery. Reusable drapes can be cost-effective if sterilization protocols are strictly followed. Disposable instruments may be used when resources allow.
3. Timeout Verification
A structured surgical timeout checklist must confirm patient identity, correct eye, procedure, and IOL power. The WHO surgical safety checklist can be adapted to cataract surgery.
4. Anaesthesia
The anaesthesia approach should reflect patient needs and surgeon expertise. Topical anaesthesia is considered safe and cost-effective. Surgeons must be properly trained in peribulbar and retrobulbar techniques.
When general anaesthesia is used, trained personnel and resuscitation equipment must be available.
5. Surgical Technique
Phacoemulsification, small-incision cataract surgery, and extracapsular extraction are all acceptable techniques. Selection depends on clinical factors, available resources, and surgeon expertise.
6. Intracameral Antibiotics
Intracameral antibiotics are recommended as standard practice to reduce endophthalmitis risk. Cefuroxime and moxifloxacin are considered equally effective. Commercial preparations are preferred over compounded formulations when available.
7. Managing Complications
Intraoperative complications must be documented and monitored. Facilities should have clear management protocols and access to vitreoretinal support within 24 hours when required. Case complexity should match surgeon experience.
III. Postoperative Phase. Outcomes, Monitoring and Continuous Improvement
The final phase closes the quality loop and determines whether effective coverage is truly achieved.
1. Postoperative Medications
Topical antibiotics are standard practice after surgery. Steroid drops are routinely used, with tapering regimens recommended to minimize steroid-induced complications.
High-risk patients may benefit from combined steroid and NSAID therapy.
2. Structured Follow-Up
Typical follow-up includes:
- 24 to 48 hours for wound integrity and inflammation
- 1 week for visual acuity and intraocular pressure
- 4 to 6 weeks for final visual acuity and refractive correction
High-risk patients require closer monitoring.
3. Measuring Outcomes
Facilities should integrate postoperative visual acuity data into health information systems. Patient-reported outcome measures and satisfaction surveys should complement objective measures.
The WHO benchmark recommends that at least 80 percent of patients achieve presenting visual acuity of 6/12 or better at 4 to 12 weeks postoperatively.
4. Postoperative Complications
Patients must receive clear instructions regarding warning signs such as pain, redness, or sudden vision loss. Rapid referral pathways should be established.
From Volume to Value
The WHO recommendations underscore a critical shift. Cataract surgery quality is not defined by surgical volume alone. It is defined by structured systems, evidence-based protocols, documented outcomes, and continuous monitoring.
For countries aiming to reach the 2030 effective coverage target, the greatest opportunity may lie not only in expanding access, but in tightening the quality architecture around every step of care.
When preoperative assessment is meticulous, intraoperative standards are uncompromising, and postoperative outcomes are tracked and audited, cataract surgery becomes more than a procedure. It becomes a high-value, system-level intervention capable of transforming lives at scale.
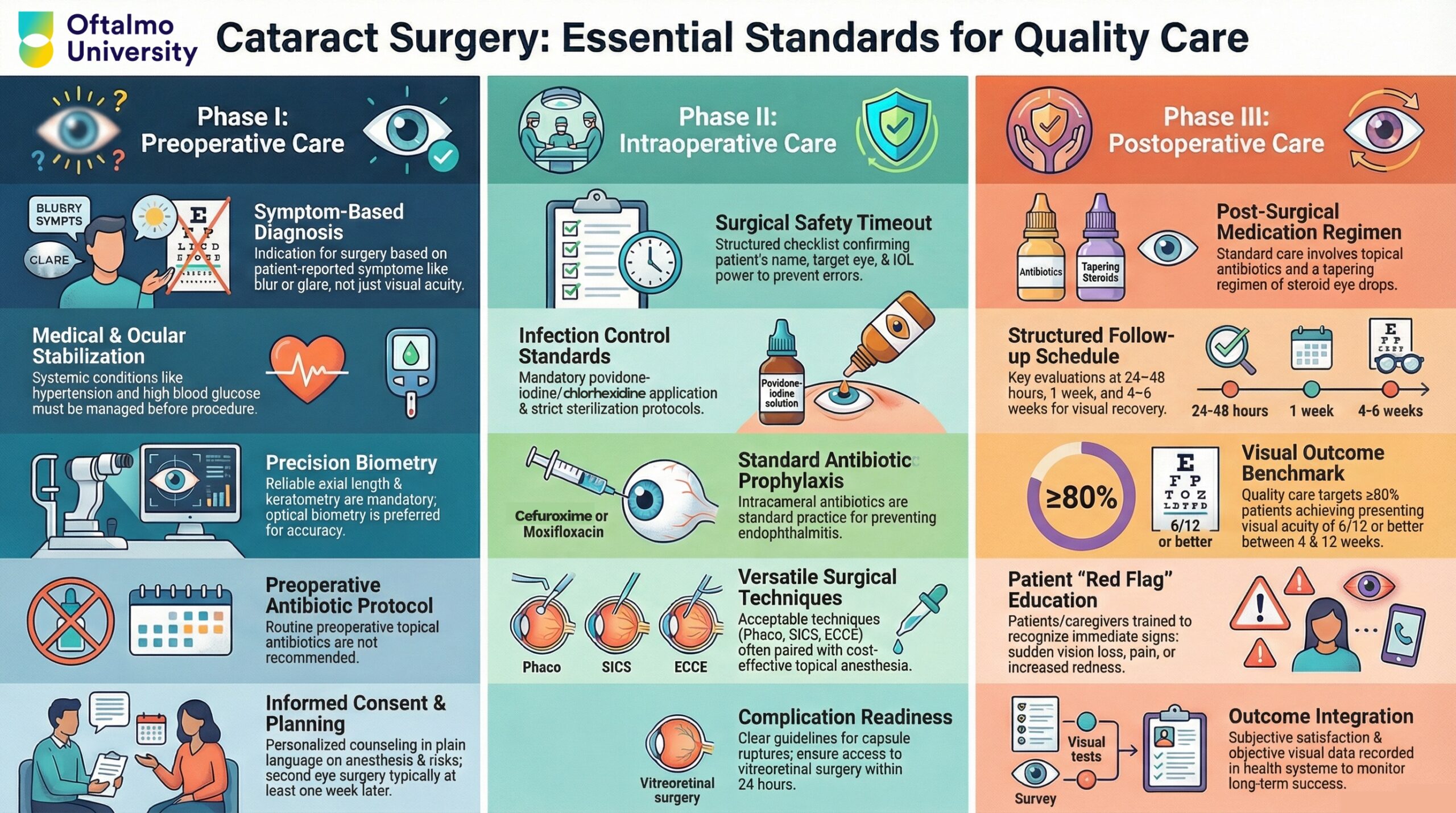
Visual Summary:
Source: WHO – Iris https://iris.who.int/items/c0a4d475-334b-4f55-9660-c02af389f9d3