Postoperative Protocols for Complicated Cataract Surgery
A Structured Approach to Risk Mitigation and Visual Rehabilitation
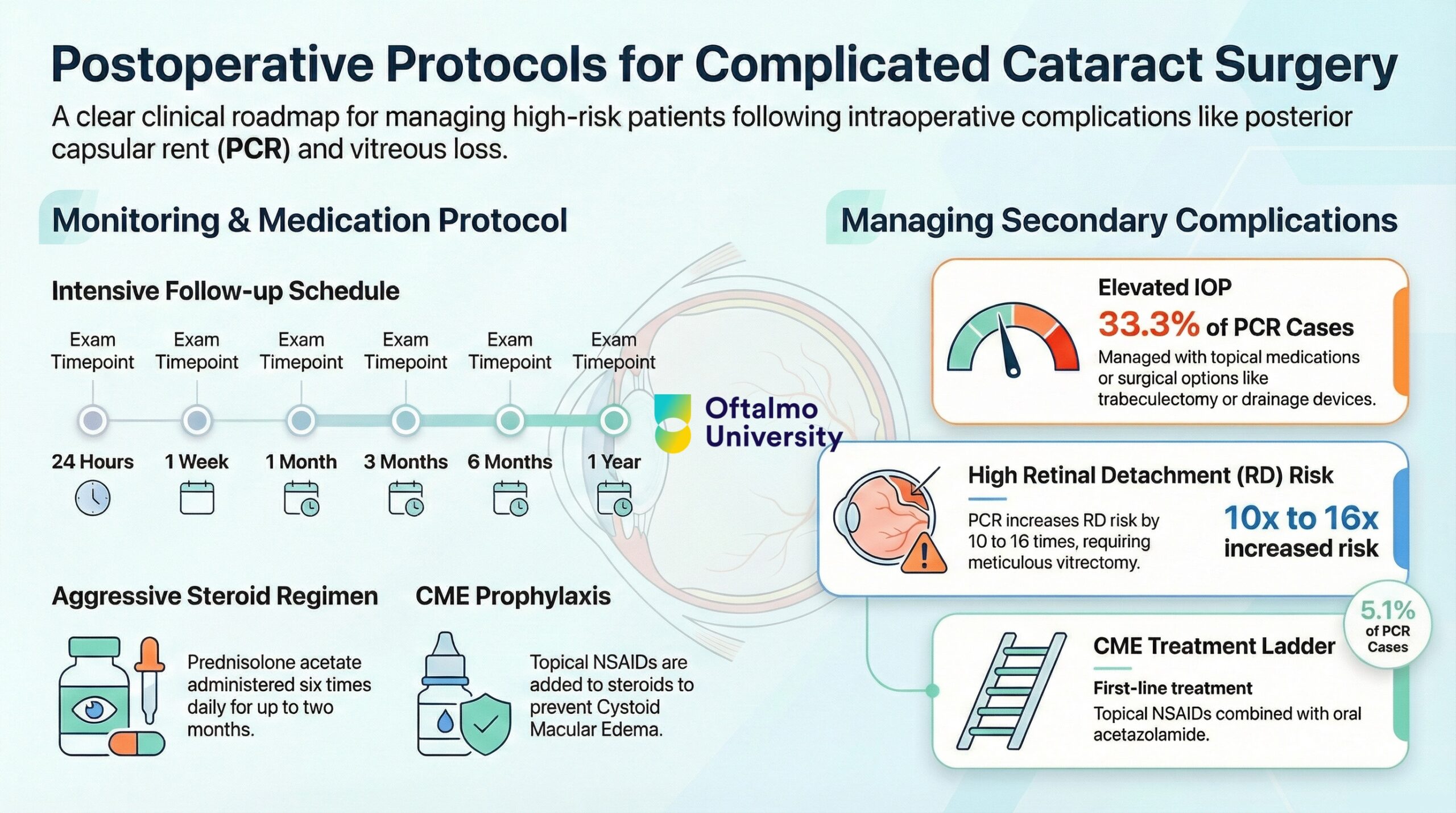
Complicated cataract surgery, particularly cases involving posterior capsular rent (PCR), vitreous loss, and anterior vitrectomy, requires a fundamentally different postoperative strategy compared to routine procedures. These patients must be considered high risk from day one. Their management demands structured surveillance, aggressive anti-inflammatory therapy, and early detection of secondary complications.
This article summarizes key recommendations for optimizing outcomes after intraoperative complications.
Follow-up Protocols. Intensified Surveillance Is Mandatory
Patients with PCR or vitreous loss require closer monitoring than standard cataract cases.
Recommended Follow-up Schedule
- First visit within 24 hours
- 1 week
- 1 month
- 3 months
- 6 months
- 1 year
Each visit should include:
- Interval history focused on new symptoms
- Visual acuity assessment
- Intraocular pressure measurement
- Slit-lamp biomicroscopy
- Dilated fundus examination
The primary goal is early detection of inflammation, pressure spikes, cystoid macular edema, or retinal pathology.
Postoperative Medication. More Aggressive Than Routine Cases
Complicated surgery induces a stronger inflammatory cascade. Medical therapy must reflect this increased risk.
Corticosteroids
- Intensive topical steroid regimen, often six times daily
- Duration may extend up to two months
- Taper guided by inflammation and corneal status
NSAIDs
- Used alongside steroids to reduce risk of Cystoid Macular Edema (CME)
- May continue for one month, especially in cases involving iris manipulation
Antibiotics
- Topical fluoroquinolones, typically four times daily
- Duration: 1 to 4 weeks
Cycloplegics
- Long-acting agents post-vitrectomy
- Provide additive anti-inflammatory and comfort benefits
The therapeutic philosophy is proactive inflammation control rather than reactive management.
Management of Key Postoperative Complications
A. Intraocular Pressure Elevation
IOP elevation is one of the most common early complications after PCR.
Early phase
- Transient spikes
- Managed with topical antiglaucoma medications
Late phase
- Persistent elevation may indicate secondary glaucoma
- Possible mechanisms: peripheral anterior synechiae or vitreous incarceration
Surgical escalation
- Trabeculectomy with mitomycin C
- Glaucoma drainage devices
- Be cautious in aphakic eyes due to risk of tube occlusion by vitreous
Early differentiation between transient and structural causes is critical.
B. Cystoid Macular Edema (Irvine–Gass Syndrome)
CME is a major cause of postoperative visual decline in complicated cases.
First-line therapy
- Topical NSAIDs
- Oral acetazolamide to enhance retinal pump function
Refractory cases
- Intravitreal dexamethasone implant
- Subtenon triamcinolone
Prompt recognition and escalation prevent chronic structural damage.
C. Retained Lens Fragments
Management depends on size and composition.
Observation
- Small cortical or nuclear chips
- Often resorb spontaneously
Surgical intervention
- Large fragments or dropped nucleus
- Pars plana vitrectomy, usually within one week
- Some surgeons prefer short delay to allow corneal clarity and better visualization
Timing balances inflammation control with surgical safety.
D. Retinal Tears and Detachment
PCR increases the risk of retinal detachment up to 10 to 16 times.
Prevention
- Thorough anterior vitrectomy
- Complete clearance of vitreous from incisions
Monitoring
- Careful peripheral retinal examination
- Patient education regarding warning symptoms such as flashes and floaters
Education becomes part of postoperative risk mitigation.
Intraocular Lens Rehabilitation Strategy
When primary IOL placement is not feasible, secondary rehabilitation must be carefully planned.
If Anterior Capsule Is Intact
- Three-piece IOL in the sulcus
- Optic capture through the capsulorhexis enhances stability
If No Capsular Support
Options include:
- Iris-fixated IOLs
- Scleral-fixated IOLs
- Sutureless techniques such as the Yamane method
- Sutured fixation techniques
The decision depends on ocular anatomy, surgeon expertise, and long-term stability considerations.
Strategic Perspective. From Complication to Controlled Recovery
Complicated cataract surgery is not the end of predictability. It is the beginning of a new algorithm.
Success depends on:
- Structured follow-up
- Aggressive inflammation control
- Early identification of secondary pathology
- Thoughtful visual rehabilitation
With a disciplined postoperative protocol, visual outcomes can remain excellent even in the presence of intraoperative adversity.
The difference between complication and catastrophe is rarely the intraoperative event itself. It is the quality of postoperative management that follows.
Visual Summary